Factors Influencing Depression among the Elderly in Island Regions
Abstract
The purpose of this study is to identify factors influencing depression among elderly people in island regions. To achieve this research objective, the study used raw data from the “Community Health Survey 2021” conducted by the Korea Disease Control and Prevention Agency. Its actual analysis was based on raw data from the “Community Health Survey 2021”, targeting 450 elderly people aged 65 or older residing in Sinan-gun, Jeollanam-do, surveyed by Sinan-gun Public Health Center. In addition, a regression analysis was performed using SPSS version 29.0 to test the research hypotheses. The results of verifying the research hypotheses showed that gender, economic activity, pain, subjective health, and subjective stress would have significant effects on depression among elderly people in island regions. Based on these research findings, various practical and policy recommendations were presented to help manage depression among the elderly in island regions.
Keywords
elderly people in island regions, depression, Andersen model, predisposing factor, enabling factor, need factor
1. Introduction
South Korea currently encounters various social problems due to rapid population aging. In particular, depression among Korean elderly people, which results from retirement, isolation from interpersonal relationships, poverty, and deteriorating health, is emerging as a major public health problem. According to a study by the Ministry of Health and Welfare and the Korea Institute for Health and Social Affairs (2020), the prevalence of depression among the elderly in South Korea was estimated at 13.5%. The problem here is that there is a rapid increase in the number of elderly people suffering from depressive disorders. Kang Seon-woo, a member of the National Assembly of Korea, analyzed data from the Health Insurance Review and Assessment Service and explained that between 2010 and 2019, the number of elderly people experiencing episodic and recurrent depressive disorders increased by 58% from 195,648 to 309,749 (Medifonews, 2020-10-08).
To address this rapidly increasing rate of depression in the elderly, the government and academia have made various interventions. The government has established mental health and welfare centers by region and operated depression management programs. In specific, Gyeonggi Province operates the “Depression Treatment Cost Support for the Elderly” project, providing up to 360,000 won per person annually for outpatient care expenses. In addition, academic circles are actively engaged in research to identify the causes of geriatric depression using various models. Notably, it has been proven in academic circles that the ‘Andersen model’ can systematically analyze depression in the elderly. In this context, the present study aims to analyze factors influencing depression among the elderly in island regions by using the Andersen model.
The Anderson model was originally a model for analyzing the “Behavioral Model of Health Service Utilization” (Andersen & Newman, 2005). However, as Andersen (1995) pointed out, medical sociologists, medical economists, and psychologists modified the Anderson model for their own use. Among the various modified models, the present study adopted a model that replaced the variable of “health service use” with “depression”, and previous studies (Park & Seo, 2019; Kim, 2016; Kang & Boo, 2010; Song & Won, 2014; Song, 2013) have also proven the effectiveness of this modified model.
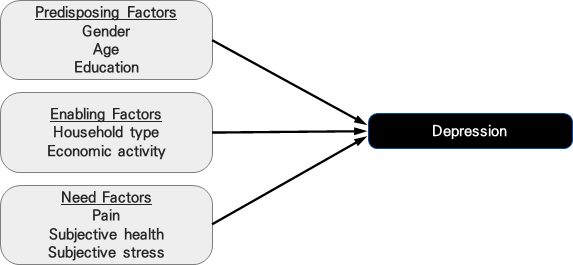
Andersen (1995) classified predictive factors influencing the dependent variable into predisposing, enabling, and need factors. Based on a review of previous studies, this study reported that predisposing factors such as gender (Kang & Boo, 2010), age (Song & Won, 2014), and education (Kang & Boo, 2010) were significantly associated with depression. Enabling factors such as household type (Jang, 2008) and economic activity (Song, 2013) were also found to significantly affect depression. In addition, the study noted that need factors such as pain (Park & Seo, 2019), subjective health (Park & Seo, 2019), and subjective stress (Park & Seo, 2019) are significantly related to depression.
Accordingly, based on the Andersen model, this study intends to analyze the effects of predisposing, enabling, and need factors on depression among elderly people in island regions. Based on the analysis results, this study also aims to provide basic data that will serve as the foundation for social welfare policies and practices to manage depression among the elderly in island regions.
2. Theoretical Background
2.1 Depression
Although the concept of depression is commonly experienced in the course of daily life, it is difficult to define the concept in a single word (Kang & Kim, 2014; National Institute of Mental Health, 2021). The most representative type of depression is major depression. Major depression has a serious impact on individuals, in which they experience symptoms such as depressed mood, sleep disorders, feelings of worthlessness, fatigue, and decreased appetite for at least two weeks (National Institute of Mental Health, 2021). The DSM-IV diagnostic criterion for major depression is the occurrence of five or more successive major depressive episodes over a two-week period (American Psychiatric Association, 2000).
In relation to measuring depression, the domain of primary medical care (e.g. public health centers) uses measures such as the Beck Depression Inventory and the Hamilton Depression Rating Scale. However, these measures have limitations in terms of having many items and difficulty explaining the depressive symptoms of modern people. The measure that has overcome these limitations is the PHQ-9 (Patient Health Questionnaire-9). The PHQ-9 scale is not only convenient to measure depression, but also a measurement tool that meets the DSM-Ⅳdiagnostic criteria (Park, Choi, Choi, Kim & Hong, 2010). In addition, the severity of depression is classified into 0–4 (none), 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe), and 20–27 (severe) (Kroenke, Spitzer & Williams, 2001).
Among OECD member countries, South Korea has a relatively highly prevalence of depression. This has increased the country’s social attention to depression. This study is set to focus on depression in the elderly among various subjects. This is because the elderly generation has been identified as having a higher prevalence of depression than other generations in South Korea. According to a study by Choi (2023), which analyzed data from the 8th National Health and Nutrition Survey (2019–2020), the elderly generation was reported to have a higher prevalence of depression than other generations. Because depression in the elderly is difficult to detect, it is often not properly treated, resulting in extreme choices such as suicide. Park (1997) explained the reasons for difficulty detecting depression among the elderly as follows: Depression in the elderly not only causes cognitive declines, but also manifests as physical symptoms such as body aches or chest tightness. In addition, elderly people have little experience in complaining about their own depressed feelings. Thus, it is a reality that elderly people themselves or people around them do not recognize it properly as geriatric depression (Park, 1997). As this shows, depression in the elderly is not easy to detect because it has characteristics that are distinguished from depression in other generations.
2.2 Anderson model
Andersen developed the “Behavioral Model of Health Service Utilization” to predict and explain the use of health services. In academia, however, the “Behavioral Model of Health Service Utilization” is also described as the “Andersen Model” (Kahng, 2010). The Behavioral Model of Health Service Utilization analyzes the predictive factors that induce an individual's health service use behavior. The predictive factors proposed by Andersen can be categorized into predisposing, enabling, and need factors. Predisposing factors refer to the demographic characteristics of individuals that influence their likelihood of using health services. Enabling factors mean their abilities to use health services, in other words, socioeconomic resources, etc. (Andersen & Newman, 2005; Jeon & Kahng, 2013). Need factors indicate the presence or absence of diseases and health status that cause individuals to use health services (Andersen & Newman, 2005; Jeon & Kahng, 2013: 136; Song & Won, 2014).
In the Initial Behavioral Model (1960s), Andersen explained the paths among the variables of predisposing, enabling, and need factors and the use of health services as shown in Figure 1 (Andersen, 1995).

Andersen’s initial behavioral model caused controversy in relation to the purpose of research conduct. Andersen (1995) first explained the causal relationships among the variables of predisposing, enabling, and need factors and the use of health services. However, subsequent studies were conducted to analyze the independent influences of predisposing, enabling, or need factors on the use of health services. Consequently, regarding this controversy, Andersen (1995) explained that it is possible to conduct either studies analyzing the paths to the use of health services or studies analyzing independent influences of the three types of factors. Between two analysis methods, studies such as that by Lyons & Bhagwandeen (2023), which analyze independent influences of the three types of factors on the use of health services, are mainly conducted as shown in Figure 2.

The initial behavioral model was modified to incorporate feedback and criticism from peers, as well as new health policies and health service frameworks. However, the revised Andersen model retained its core components and their relationships, including predisposing factors, enabling factors, need factors, and the utilization of health services (Andersen, 2008).
Subsequently, Andersen (1995) published a study suggesting that the dependent variable, "use of health services," could be replaced with "health outcomes." As a result, numerous studies adopted modified versions of the model, replacing the dependent variable "use of health services" with "depression." This modification has been widely applied, and its validity has been demonstrated in previous studies (Park & Seo, 2019; Kim, 2016; Kang & Boo, 2010; Song & Won, 2014; Song, 2013).
2.3 Review of previous studies
The purpose of this study is to analyze the predisposing, enabling, and need factors as factors influencing depression among elderly people in island regions. Specific previous studies related to this topic are as follows:
First, predisposing factors refer to the sociodemographic characteristics of individuals that affect their likelihood of using health services (Andersen & Newman, 2005; Jeon & Kahng, 2013). In this study, gender, age, and education were selected as predisposing factors. In terms of gender, women were reported to have an overall higher level of depression than men. This is because women have high levels of social vulnerabilities including patriarchy and gender discrimination (Carter, Psych, Joyce, Mudler, Luty & McKenzie, 2000). Kang & Boo (2010), who analyzed elderly people aged 65 or older, pointed out that depression increases in older women. In addition, a study by Song & Won (2014), which analyzed elderly people with disabilities using the Andersen model, explained that depression increases with age. This is because people experience problems such as deteriorating health, isolation from social relationships, and economic difficulties with aging, which results in increased depression. In addition, a study by Kang & Boo (2010), which analyzed elderly people aged 65 years or older, confirmed a significant correlation between education and depression. Education levels are closely associated with an individual's socioeconomic status. In other words, elderly people with low levels of education are more likely to experience economic difficulties and social isolation, which eventually increases their risk of depression.
Second, enabling factors refer to an individual’s ability to use health services, in other words, socioeconomic resources (Andersen & Newman, 2005; Jeon & Kahng, 2013). In this study, household type and economic activity were selected as enabling factors. The reasons for this selection are as follows: According to Jang (2008), elderly people who live with their family members are reported to have lower levels of depression. This is probably because they feel protected safely by their family members, helping to reduce their depression. In addition, Song (2013) reported that economic activities reduce depression among the elderly since it gives meaning to their life. In other words, economic activities provide them with the meaning of supporting their families or contributing to society through their own efforts and capabilities.
Third, need factors mean the presence or absence of diseases and health status that cause individuals to use health services (Andersen & Newman, 2005; Jeon & Kahng, 2013: 136; Song & Won, 2014). In this study, pain, subjective health, and subjective stress were selected as need factors. The reasons for this are as follows: Pain restricts the mobility of elderly people, thereby causing their social isolation, and this increased sense of social isolation becomes a major mechanism for increasing one’s depression. According to a study by Park & Seo (2019), which analyzed data from the National Health and Nutrition Examination Survey, pain had a significant impact on depression. Moreover, subjective health has a negative impact on the self-evaluation of elderly people. In other words, when elderly people negatively perceive their own health status, it leads to an increase in their depression, which is a negative phenomenon of self-distortion. Park & Seo (2019) also pointed out that subjective health has a significant effect on depression. Stress is another factor that can induce or worsen depression. The reason is that when elderly people face a stressful situation and are unable to actively cope with it, they can feel anxious and helpless about themselves, which eventually increases their depression. Park & Seo (2019), who utilized the Andersen model for their study, noted that subjective stress has a significant impact on depression.
3. Research Methods
3.1 Research model
The purpose of this study is to identify factors that influence depression among elderly people in island regions. Based on the results of previous studies, a research model was established in this study as shown in Figure 3.
3.2 Research subjects and methods
This study utilized raw data from the “Community Health Survey 2021” conducted by the Korea Disease Control and Prevention Agency. The Community Health Survey 2021 was conducted between August 16 to October 31, 2021 through an electronic survey (CAPI: Computer Assisted Personal Interviewing) on 229,242 adults aged 19 or older nationwide. The actual analysis of this study involved 450 elderly people aged 65 or older residing in Sinan-gun, Jeollanam-do, surveyed by Sinan-gun Public Health Center, based on raw data from the ‘Community Health Survey 2021’.
To test the research hypotheses, SPSS version 29.0 was used for data analysis. To identify the characteristics of the main variables, frequency and descriptive statistical analyses were conducted. Second, a regression analysis was performed to analyze the factors that influence depression among elderly people in island regions.
3.3 Measurement Tools
1) Dependent variables
Depression was measured using the Patient Health Questionnaire-9 (PHQ-9) scale. The PHQ-9 scale is a Korean version that Park, Choi, Choi, Kim, and Hong (2010) produced by verifying the reliability and validity of its original scale developed by Spitzer, Kroenke, and Williams (1999). The PHQ-9 consists of nine items whose responses are based on a 4-point Likert scale in which 1 point denotes “not at all”, 2 points “for several days”, 3 points “for more than a week”, and 4 points “almost every day.” Therefore, a higher score means a corresponding higher level of depression. In this study, the Cronbach's alpha value was confirmed to be .766 (Korea Disease Control and Prevention Agency, 2022).
2) Independent variables
The study’s predisposing factors are gender, age, and education levels. Gender consisted of ‘male=1, female=2’, and the actual analysis employed a dummy process with ‘female=0, male=1.’ Although age is a ratio scale, it was converted into ‘under 75 years old = 1, 75 years old or older = 2’ in the frequency analysis. Education levels consisted of ‘no education = 1, seodang/Chinese studies = 2, elementary school = 3, middle school = 4, high school = 5, 2–3 year college = 6, 4-year college = 7, and graduate school or higher = 8’, and the actual analysis used a dummy process with ‘no education, seodang/Chinese studies = 0, elementary school or higher = 1’ (Korea Disease Control and Prevention Agency, 2022).
The study’s enabling factors consisted of the variables of household type and economic activity. Household type refers to the presence or absence of a spouse and was subject to a dummy-process with ‘no spouse = 0, spouse = 1.’ Economic activity was a single item asking, “Have you ever worked for more than 1 hour for income or worked as an unpaid family worker for more than 18 hours in the past week?” and its answers consisted of ‘Yes = 1, No = 2.’ However, a dummy process was used in this study with ‘No = 0, Yes = 1’ (Korea Disease Control and Prevention Agency, 2022).
The need factors consisted of the variables of pain, subjective health, and subjective stress. Pain was measured using the pain/discomfort variable of the EQ-5D. The responses were 1 point for ‘I have no pain or discomfort’, 2 points for ‘I have some pain or discomfort’, and 3 points for ‘I have very severe pain or discomfort’. Therefore, a higher score indicates a corresponding higher level of pain. Subjective health levels were measured using a single question asking, “How do you usually think about your health?” The responses were based on a 5-point Likert scale from 1 point (very good) to 5 points (very bad). In this study, this scale was converted into 1 point (very bad) to 5 points (very good). Therefore, a higher score denotes a subjective better health level. Stress was measured using a single question asking, “How much stress do you usually feel in your daily life?” The responses were based on a 4-point Likert scale from 1 point for “I feel it very much” to 4 points for “I rarely feel it.” In this study, these scores were converted into 1 point for “I hardly feel it” to 4 points for “I feel it very much”. Thus, a higher score indicates a corresponding higher stress level (Korea Disease Control and Prevention Agency, 2022).
4. Research Result
4.1 Sociodemographic characteristics of respondents
The demographic characteristics of the respondents are presented in Table 1. First, in terms of gender, the respondents consisted of women at 41.1% and men at 58.9%. In terms of age, the average age was 75.6 years old, with middle-old aged people (65–74 years old) accounting for 44.9% and old-old aged people (75 years old and older) for 55.1%. Regarding the education of the respondents, 28.6% of the respondents were uneducated and 71.4% had elementary or higher levels of education. In terms of household type, 40.2% had no spouse and 59.8% had a spouse. Regarding economic activity, 46.7% were economically active and 53.3% were not economically active.
| Category | Frequency | Percentage (%) | Other | |
|---|---|---|---|---|
| Gender | Female | 185 | 41.1 | |
| Male | 265 | 58.9 | ||
| Age | 65–74 years old (middle-aged and elderly) | 202 | 44.9 | Mean (SD) 75.6 (6.71) |
| 75 years of age or older (elderly) | 248 | 55.1 | ||
| Education | No education | 128 | 28.6 | |
| Elementary school or above | 320 | 71.4 | ||
| Household type | No spouse | 181 | 40.2 | |
| Spouse | 269 | 59.8 | ||
| Economic activity | Difficult | 210 | 46.7 | |
| Not difficult | 240 | 53.3 | ||
4.2 Descriptive Statistics of Main Variables
The descriptive statistics of the main variables are presented in Table 2. The average pain score was 1.72 (SD .66). The average subjective health score was 2.79 (SD 1.06), and the average subjective stress score was 1.75 (SD .77). The average depression score was 1.29 (SD .37).
| Category | Min | Max | Mean | SD |
|---|---|---|---|---|
| Pain | 1.0 | 3.0 | 1.72 | .66 |
| Subjective health | 1.0 | 5.0 | 2.79 | 1.06 |
| Subjective stress | 1.0 | 4.0 | 1.75 | .77 |
| Depression | 1.0 | 3.0 | 1.29 | .37 |
4.3 Hypothesis testing
The results of the analysis of factors influencing depression among the elderly in island regions are presented in Table 3. First, according to an examination of the model's goodness of fit, the F value was 21.124, and statistical significance was confirmed at the level of p<.001. When the variables of gender, age, education, household type, economic activity, pain, subjective health, and subjective stress were entered into the model, their explanatory power for depression was reported to be 26.6%. Among the predisposing factors, the variable of gender (β=.175) had a significant impact on depression, which suggests that women had an overall higher level of depression. In enabling factors, the variable of economic activity (β=.105) had a significant impact on depression. This implies that those who are economically more active are less depressed. Lastly, in need factors, the variables of pain (β=.141), subjective health (β=-.129), and subjective stress (β=.356) had significant influences on depression. This indicates that greater pain and poorer subjective health, and higher subjective stress lead to a corresponding higher level of depression.
| Category | B | S.E. | β | t | VIF | |
|---|---|---|---|---|---|---|
| Predisposing Factors | Gender | .010 | .003 | .175 | 3.557*** | 1.479 |
| Age | -.003 | .035 | -.004 | -.087 | 1.325 | |
| Education | -.045 | .039 | -.056 | -1.148 | 1.443 | |
| Enabling Factors | Household type | .008 | .035 | .011 | .233 | 1.322 |
| Economic activity | .077 | .033 | .105 | 2.317* | 1.255 | |
| Needs Factors | Pain | .078 | .026 | .141 | 3.013** | 1.336 |
| Subjective health | -.045 | .017 | -.129 | -2.634** | 1.467 | |
| Subjective stress | .169 | .021 | .356 | 8.039*** | 1.191 | |
| Constant | .252 | |||||
| F | 21.124*** | |||||
| adj. R2 | .265 | |||||
Note) Dummy: Gender (male = 1), Education (elementary school or higher = 1), Household type (spouse = 1), Economic activity (economically active = 1)
5. Conclusion
The purpose of this study is to analyze the effects of predisposing, enabling, and need factors on depression among the elderly in island regions based on the Andersen model. The results of the study are as follows:
First, in terms of predisposing factors, gender had a significant effect on depression among elderly people in island regions. This is consistent with the findings of a previous study (Kang & Boo, 2010). The reason for such high levels of depression among elderly women is because elderly women in island regions experience high levels of social vulnerabilities such as patriarchy and gender discrimination (Carter, Psych, Joyce, Mudler, Luty & McKenzie, 2000). Therefore, various practical strategies are required to reduce depression in elderly women residing in island regions. First, programs in the form of various self-help groups should be implemented to reduce depression among elderly women in island regions. Furthermore, it is urgent to introduce educational programs and psychological counseling sessions to address issues related to patriarchy and gender discrimination in these areas.
Second, in terms of enabling factors, economic activity was reported to have a significant effect on depression among the elderly in island regions. This is in line with the results of a previous study (Song, 201). The reason behind this relationship is that a person’s economic activities not only enable the acquisition of resources, but also provide the meaning of supporting their family or contributing to society (Song, 2013). Thus, it is necessary to develop policies that promote economic activities of the elderly in island regions. In other words, it is needed to develop and expand employment projects for the elderly, which take into account the characteristics of elderly people in island regions. Moreover, given that elderly residents in island regions are often engaged in economic activities due to their economic difficulties, it is necessary to consider income guarantee policies such as the expansion of basic pensions.
Third, regarding needs factors, the variables of pain, subjective health, and subjective stress had significant effects on depression in the elderly. This is aligned with the results of a previous study (Park & Seo, 2019). First, in terms of the relationship between pain and depression, pain is likely to increase depression among elderly people in island regions because it restricts their mobility and causes social isolation. Hence, it is necessary to develop and operate outreach programs that can manage pain in elderly people in island regions at public health centers. In terms of the relationship between subjective health and depression, if elderly people negatively perceive their own health status, they are likely to experience increased depression, a negative self-distortion phenomenon. In other words, along with regular checkups for elderly people in island regions, it is recommended to develop and operate customized health promotion programs. Lastly, regarding the relationship between subjective stress and depression, if elderly people in island regions cannot actively cope with their stressful situations, they can feel anxious and helpless about themselves, which can ultimately increase their depression. Therefore, it is necessary to regularly deploy professional psychological counselors and programs in island regions or utilize remote counseling services to provide psychological stability.
The limitations of this study lie in its focus on elderly individuals aged 65 and over in Shinan County, making it difficult to generalize the findings to the elderly population nationwide. Future studies should include analyses targeting elderly individuals across the country, along with comparative studies between elderly residents in island regions and urban areas to identify the unique characteristics of depression experienced by island residents. In addition, this study was conducted as a quantitative study. Therefore, qualitative research is necessary in the future to make more multifaceted approaches that can address topics that are hard to clarify through statistical data.
Acknowledgements
This Research was supported by Research Funds of Mokpo National University in 2023.
References
- American Psychiatric Association, 2000. Diagnostic and Statistical Manual of Mental Disorders.(4th Text Revision ed.) Washington, DC: American Psychiatric Association.
- Andersen, R., Newman, J.F., 2005. Societal and Individual Determinants of Medical Care Utilization in the United States. Milbank Quarterly. 83(4): 1–28.
- Andersen, R.M., 1995. Revisiting the Behavioral Model and Access to Medical Care: Does it Matter?. Journal of Health and Social Behavior. 36(1): 1–10.
- Andersen, R.M., 2008. National Health Surveys and the Behavioral Model of Health Services Use. Medical Care. 46(7): 647–653.
- Carter, J.D., Psych, D.C., Joyce, P.R., Mudler, R.T., Luty, S.E., McKenzie, J., 2000. Gender differences in the presentation of depressed outpatients: a comparison of descriptive variables. Journal of Affective Disorder. 61(1–2): 59–67.
- Choi, K.J. 2023. Changes in the prevalence of depression in adults due to the COVID-19 Pandemic: Data from the 8th (2019~2020) National Health and Nutrition Examination Survey. Journal of the Korea Academia-Industrial cooperation Society. 24(5): 529–537.
- Jang, S.M.. 2008. Family Type and Family Support Effecting on Depression of Elderly Diabetics. Korean Journal of Family Social Work. 22: 35–66.
- Jeon, H.S., Kahng, S.K., 2013. A Study on age differences in the trajectory of outpatient service use among individuals participating in Korean Welfare Panel Study on Disability. Korean Journal of Social Welfare Research. 34: 133–159.
- Kahng, S.K., 2010. The Trajectory of Outpatient Medical Service Use and Its Predictors: Focusing on Age Variations. Korean Journal of Social Welfare. 62(3): 83–108.
- Kang, S.K., Boo, K.C., 2010. Predictors of Elderly Depression Using the Andersen Model. Journal of Welfare for the Aged. 49: 7–30.
- Kang, U.G., Kim, H.S., 2014. A Historical Consideration of Psychiatric Diagnostic Systems : Focusing on the Concept of Depression. JOURNAL OF THE KOREAN NEUROPSYCHIATRIC ASSOCIATION. 53(5): 259–292.
- Kim, J.K., 2016. Effect of Public Pension on Depression among Korean Older Adults:The Differences between Poor and Non-poor Households. Korean Journal of Gerontological Social Welfare. 71(4): 423–447.
- Korea Disease Control and Prevention Agency, 2022. Guidelines for Using the 2021 Community Health Survey Raw Data.
- Kroenke, K., Spitzer, R.L., Williams, J.B., 2001. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine. 16(9): 606–13.
- Lyons, N., Bhagwandeen, B., 2023. Examining healthcare needs and decisions to seek health services among Venezuelan migrants living in Trinidad and Tobago using Andersen’s Behavioral Model. Frontiers in Public Health. 1–16. (DOI 10.3389/fpubh.2023.1212825)
- Medifonews (2020-10-08). Assemblywoman Kang Sun-woo: "Elderly with Mental Illness Increased by 81% Over the Last 10 Years". (Newspaper article)
- Ministry of Health and Welfare and the Korea Institute for Health and Social Affairs, 2020. 2020 Elderly Survey(Survey)
- National Institute of Mental Health, 2021. Depression.
- Park, H.E., Seo, I.S., 2019. Factors Affecting Depression in the Elderly Over 65 Years in Korea: Using Andersen's Behavioral Model. Journal of the Korea Convergence Society. 10(8): 83–95.
- Park, J.H., 1997. Characteristics of Depression in the Aged People. Journal of the Korean Society of Biological Therapies in Psychiatry. 3(1): 14–20.
- Park, S.J., Choi, H.R., Choi, . J.H., Kim, K.W., Hong, J.P., 2010. Reliability and Validity of the Korean Version of the Patient Health Questionnaire-9 (PHQ-9). Anxiety Mood. 6(2): 119–124.
- Park, S.J., Choi, H.R., Choi, J.H., Kim, K.W., Hong, J.P., 2010. Reliability and Validity of the Korean Version of the Patient Health Questionnaire-9 (PHQ-9). Anxiety and Mood. 6(2): 119–124.
- Song, I.U., Won, S.J., 2014. Factors Affecting Depression of Older Adults with Disability Applying Andersen Model. Journal of Rehabilitation Research. 18(3): 23–45.
- Song, T.M., 2013. An Anderson Model Approach to the Mediation Effect of Stress-Vulnerability Factors on the Use of Outpatient Care by the Elderly. Health and Social Welfare Review. 33(1): 547–576.
- Spitzer, R.L, Kroenke, K., Williams, J.B., 1999. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 282(18): 1737–1744.